A Translational Preclinical Strategy for Chronic Spinal Cord Injury: Neuroprotective and Regenerative Potential of Botulinum Neurotoxin Type A combined with Muscle Atrophy Prevention via Electrostimulation
A Translational Preclinical Strategy for Chronic Spinal Cord Injury: Neuroprotective and Regenerative Potential of Botulinum Neurotoxin Type A combined with Muscle Atrophy Prevention via Electrostimulation
Mastrorilli, V.; Luvisetto, S.; Ruggieri, V.; Raparelli, G.; Madaro, L.; Paggi, L. A.; Parisi, C.; De Santa, F.; De Angelis, F.; D'Elia, A.; Massari, r.; Amadio, S.; Rossetto, O.; Vacca, V.; Caruso, M.; Sferrazza, G.; Pavone, F.; Marinelli, S.
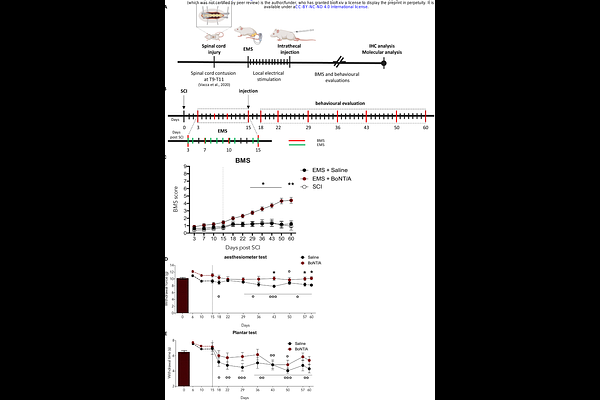
AbstractBackground: Spinal cord injury (SCI) triggers persistent neuroinflammation, gliosis, neuronal loss, and demyelination, leading to motor deficits and neuropathic pain. Botulinum neurotoxin type A (BoNT/A) has shown anti-inflammatory and neuroprotective effects in acute SCI, but its potential in the chronic phase remains unclear. This study investigates whether combining BoNT/A with electrical muscle stimulation (EMS) enhances recovery in chronic SCI. Methods: Adult mice with severe thoracic SCI (paraplegic) underwent EMS (30 min/day for 10 non-consecutive days starting 3 days post-injury) or no stimulation. Fifteen days after SCI, animals received a single intrathecal injection of BoNT/A (15 pg/5 L) or saline. Functional recovery was assessed up to 60 days as well as in moderate and mild SCI mice, neuropathic pain onset and maintenance were evaluated. Spinal cord tissue was analysed for astrocytic and microglial morphology, neuronal and oligodendroglia survival, myelin protein expression, and in vitro effects on oligodendrocyte precursor cells (OPCs). The phenotype of hindlimb muscles was evaluated through morphological and gene expression analyses. Results: EMS was able to counteract muscle atrophy and fibrosis, and when combined with BoNT/A, also denervation. Moreover, the combination restored hindlimb motor function in chronic SCI, whereas BoNT/A or EMS alone were ineffective. Neuropathic pain, a common comorbidity associated with SCI, was mitigated by BoNT/A treatment even when administered in the chronic phase. BoNT/A reduced astrocytic hypertrophy and excitatory synapse association and was associated with a morphology-based redistribution of microglial profiles toward a resting-like classification, decreased apoptosis, and increased neuronal and oligodendroglia survival. Myelin basic protein expression was significantly elevated in vivo. In vitro, BoNT/A promoted OPC differentiation into myelinating oligodendrocytes, increased process complexity, and upregulated Myelin basic protein, galactocerebroside C, proteolipid protein, and myelin oligodendrocyte glycoprotein under both proliferative and differentiating conditions. Cleaved SNAP25 colocalization with OPC confirmed direct BoNT/A internalization and activity. Conclusions: BoNT/A exerts multi-cellular neuroprotective actions in chronic SCI, supporting neuronal and oligodendroglia survival, reducing neuroinflammation, enhancing remyelination and the combination with EMS promotes substantial recovery of muscle homeostasis within a permissive microenvironment shaped by early stimulation. Its efficacy depends on a permissive microenvironment achieved through EMS. These results provide strong rationale for the clinical evaluation of BoNT/A as a therapeutic strategy for chronic SCI.